🧬
Evolution of telemedicine in India (govt vs private)
Now telemedicine in India didn't evolve because doctors demanded it. It is because there was a lack of access between the patient and the doctor, especially in tier two and tier three cities. Around the beginning of 2018, especially in India, we saw a lot of emerging applications that took the first wave of problems, basically bridging the gap between the doctor and the patient by providing a platform for patients to search doctors near their location. This helped in discoverability and visibility of doctors. Moreover, from an infrastructure standpoint, doctors didn't have a way to promote themselves. They were confined to their own clinics, and the only source of income was local patients.
Now in early 2019–2020, we saw a lot of venture capitalists start funding startups that were trying to solve the problem of creating good infrastructure.
The government came up with eSanjeevani, which is a national telemedicine service for people in India. It is a step towards digital healthcare equity to achieve universal health coverage. It not only bridged the gap but also facilitated easy access to doctors and medical experts from the patient's smartphone. It was launched by the Ministry of Health and Family Welfare (MoHFW) to address critical challenges in the healthcare system, such as shortage of doctors, lack of continuity in medical records, and overburdening of hospitals.
India's digital health ecosystem has also witnessed rapid growth in private telemedicine companies. These include Practo, 1mg, mFine, etc. They serve both doctors as well as patients. They combine teleconsultation with an extensive online pharmacy and AI symptom checker. Some of these applications also include individual and corporate wellness. While many of them leverage AI infrastructure to assist diagnosis and also integrate wearable health tracking systems. There are applications that also emphasize home healthcare for the elderly and people who are chronically ill. Overall, these platforms do not divide the main focus, but complement national efforts like eSanjeevani.
Private players approached it as convenience plus monetization. Faster consultations, urban-first adoption, and retention through subscriptions. As I have covered in the real story of online doctor consultation in India, they follow a subscription-based model where doctors have to pay a certain amount. If a patient is booked through the platform, that amount is deducted from their wallet, and if not, it is refunded back. That is the subscription model they follow.
Now what has actually happened is that the government solved the reachability issue, and the private players solved the experience issue. Neither has solved continuity of care properly. That's still widely open.
Real use cases (where it actually works vs where it pretends to)
Now let's be honest. Telemedicine applications are not a universal layer. It mainly solves the communication issue. There are certain aspects where it works beautifully. For example, follow-ups. This is the biggest no-brainer where it has solved a big chunk of the problem. Chronic disease management, for example blood pressure, diabetes, etc. It has also solved first-level triage, such as fever, cold, minor infections, and mental health consultations, since they are highly dependent on conversation and communication between the therapist and the patient.
Now coming to where it actually fails: anything needing touch, palpation, and auscultation; multi-symptom ambiguous cases; elderly patients who can't articulate symptoms properly. The reality is that telemedicine has not replaced consultation, especially physical consultation. It is filtering which patient deserves in-person time. That's a very different job.
Cost vs traditional consultation
On paper, telemedicine consultations are cheaper, which is due to the fact that it is done mostly online. The cost of bridging the gap between the patient and the doctor is quite low compared to physical consultations. But that's a shallow way of looking at it.
From the patient's perspective, it saves a lot of travel time, reduces opportunity cost, and provides faster access. From the doctor's perspective, it has lower marginal cost per consultation, higher volume potential, but lower depth per interaction.
Now what is the hidden trade-off? You reduce cost per consultation, but on the other hand, it increases repeat consult probability because uncertainty is higher. So you end up with cheaper visits but potentially more visits.
Legal framework — simplified (and what it really means)
In the Indian context, telemedicine has the potential to increase access for all Indians, given that the doctor-to-patient ratio is low. To be exact, around 811 Indians have only one doctor. This creates a huge gap and an inequitable distribution of healthcare services, which has been a major goal in public healthcare management for years. The disparity is even more visible in rural areas because more doctors prefer to practice in cities.
In the 2020 guidelines under the Medical Council of India, which is now governed by the National Medical Commission, the non-bureaucratic version is this: you can consult remotely, you can prescribe within limits, you must document everything, and you are fully responsible for outcomes.
So the law is not restrictive. It is deliberately open-ended. This means good doctors feel cautious about using the platform, and bad actors exploit the system. The law in India gives permission, but it doesn't give protection.
In one of the recent cases in Feb 2026, fake AI-generated prescriptions surfaced, where the All India Organisation of Chemists and Druggists (AIOCD) formally wrote a letter to the PM's office stating that AI-generated fake prescriptions are in the market and are reportedly being accepted by unregulated e-pharmacies. The regulatory loopholes exploited by e-pharmacies are covered under GSR 817(E) and GSR 220(E) notifications, which allow the sale of online drugs and cosmetic medications and promote home delivery. The AIOCD argued that these platforms not only misuse these provisions but also promote a false AI-generated prescription ecosystem, which can seriously compromise patient safety.
What doctors can and cannot do (practical interpretation)
Now forget about the PDF guidelines. Here's how it plays out in real life. From the doctor's perspective, you can treat low-risk, high-probability conditions, continue existing treatment, and use judgment based on history. This works well for low-risk symptoms such as fever or mild headache.
But they also say that you should avoid using telemedicine platforms for first-time diagnosis of complex cases. Also avoid aggressive prescribing without physical validation and overconfidence in patient-reported data, because there are high chances that this data may be fabricated, or the patient may not fully understand what the prescription implies.
The real constraint is not legal, it's epistemic: "Do I really know enough to treat this patient?" Telemedicine forces humility or exposes the lack of it.
Prescription legality (and why it's more serious than offline)
There is no doubt that prescriptions are legal, and it is one of the dire needs in this telemedicine market space, especially in India where people speak multiple languages and often cannot read a doctor's handwritten prescription. That is why there was a need for digitally generated prescriptions in a clear written format so that they can be understood by both the patient and the pharmacist.
Drug categories like List O, A, B, etc. exist, but most platforms blur this in practice. What it actually comes down to is: are you prescribing defensively? Can you justify this without a physical examination?
In OPD (Outpatient Department), judgment is often implicit. In telemedicine, it becomes evidence.
Comparison: eSanjeevani vs private platforms
Now that's where the huge gap is. It's not just product versus product, it's philosophy versus philosophy.
eSanjeevani
It is built for scale, not delight. Doctor availability is prioritized over doctor choice. It works best in assisted settings such as PHCs and with health workers. (Telemedicine in India — impact analysis)
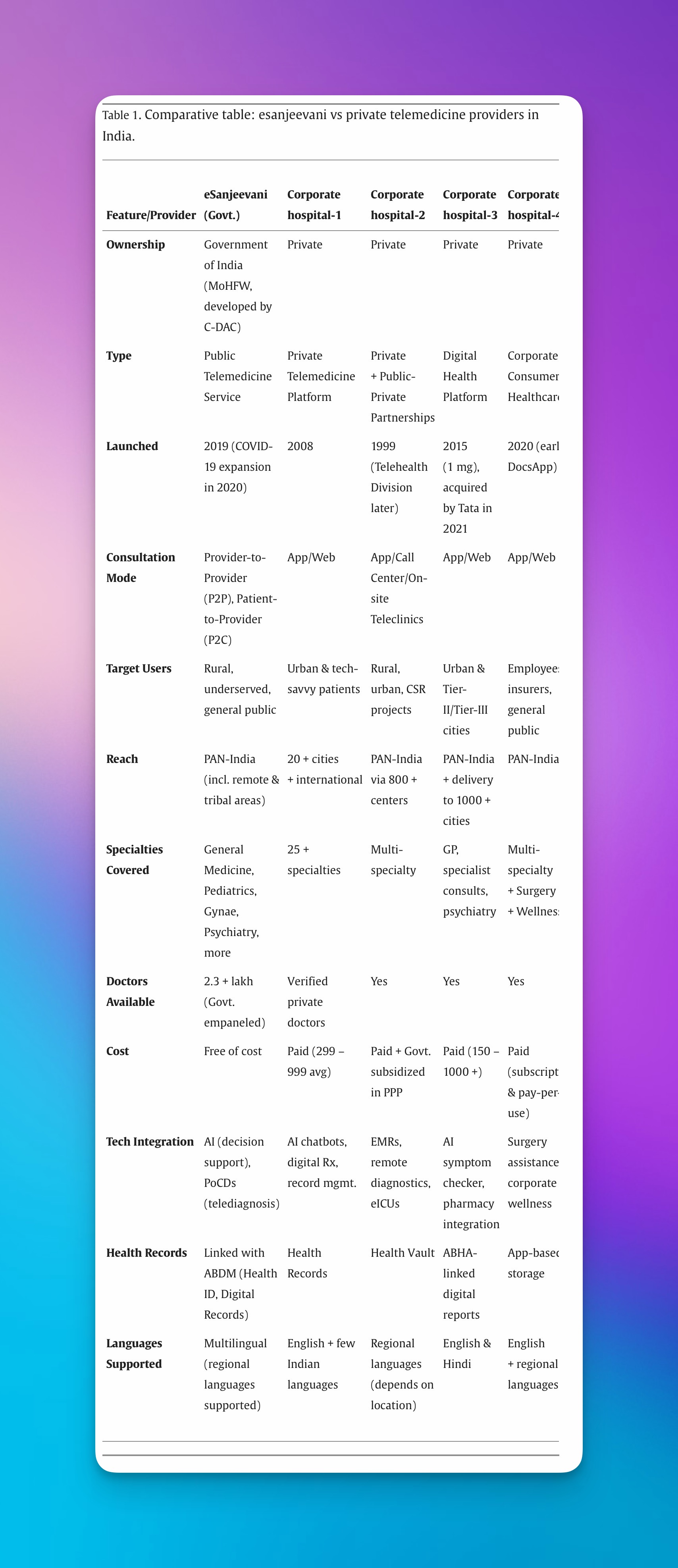
Private platforms
Private platforms, on the other hand, are built for user experience and retention. Patients choose doctors based on filters such as location, price, and experience. It focuses on a faster, smoother, and more predictable experience.
Now here is the key gap: the government lacks personalization, and the private sector lacks affordability at scale.
Limitations nobody talks about
The deeper issues that nobody talks about include the symptom storytelling problem. Patients are bad narrators, and telemedicine depends entirely on narration.
Another problem is over-standardization. Platforms push doctors into templates, which reduces nuanced thinking. They may not go beyond what has already been structured by the platform.
There is also doctor fatigue at scale. Back-to-back, low-context consultations promote cognitive burnout.
Then there are misaligned incentives. Platforms optimize for completion rate, not diagnostic accuracy. These are the metrics that don't show up in marketing decks, but they define outcomes.
Risks (clinical, operational, reputational)
Clinically, there are missed red flags and delays in escalation because the doctor doesn't really know what's happening with the patient after the consultation ends. There is no continuous feedback loop.
Operationally, there is weak documentation and identity mismatch. Although there are guardrails set by platforms to verify doctors, some actors bypass these guardrails and pretend to be legitimate practitioners.
Reputationally, one bad case can be amplified online. Trust erosion is faster than trust building.
Telemedicine compresses time but expands consequences.
Contrarian #1 — Telemedicine is not replacing doctors, it is filtering
In my opinion, telemedicine is not a doctor replacement, and AI is not going to take over anytime soon. It acts as a triage layer and a time allocation system. It decides which doctor is needed, what kind of expertise is required, and how urgently it is needed.
Doctors who adapt will see fewer but higher-value cases and spend less time on noise. Doctors who don't will end up competing in a race to the bottom on quick consults.
Contrarian #2 — Legality is not the biggest barrier, trust is
Now if you search whether it is legal or not, that problem is already solved. The real questions are: will patients trust a remote diagnosis? Will doctors feel safe making one? Will platforms prioritize care over conversion?
These are the important questions we need to address. One of the key issues we still face with telemedicine applications is generic prescriptions. They are not tailored to the patient's context or language. Many patients are still not aware of what is written in prescriptions, even though they are digitally generated, because they are written in highly technical language.
There is also a lack of follow-up. These are the important breaking points that need to be solved in the next generation of telemedicine applications.
Read next: Real story of online doctor consultation in India — a deep dive into how the actual patient journey plays out across marketplace, pooled, and doctor-owned telemedicine models.
Share this article

Rittam Debnath, FOUNDER
Rittam is the founder of Medichat, building AI-powered communication tools for private doctors in India and the UK. He writes about the future of digital healthcare, clinical workflow automation, and what it actually takes to build infrastructure for independent medical practices at scale.
Try MediAI Free for 14 Days
Built for Indian private practitioners. No credit card required. Doctor approval on every message.